




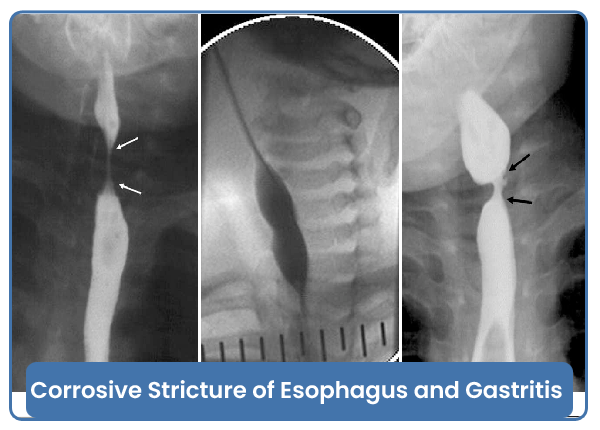
Corrosive Stricture of Esophagus and Gastritis
Corrosive stricture of the esophagus is a condition in which the esophagus narrows due to scarring and inflammation caused by the ingestion of corrosive substances, such as strong acids or alkalis. This condition can result from accidental ingestion of household or industrial chemicals and is a medical emergency requiring prompt evaluation and intervention.
Key Points about Corrosive Stricture of the Esophagus:
-
Causes: Corrosive strictures are typically caused by the ingestion of corrosive substances, including strong acids (e.g., sulfuric acid) or alkalis (e.g., lye or caustic soda). Ingestion can lead to severe tissue damage and scarring.
-
Symptoms: Individuals with corrosive stricture may experience difficulty swallowing (dysphagia), chest pain, weight loss, regurgitation, and recurrent respiratory infections.
-
Diagnosis:
- Endoscopy: Direct visualization of the esophagus using a flexible tube with a camera allows for the assessment of the extent of damage and the presence of strictures.
- Esophageal Manometry: Measures pressure and motility of the esophagus.
- Barium Swallow: X-ray imaging using a contrast material to highlight the esophagus and detect strictures.
-
Treatment:
- Dilation (Esophageal Bougienage or Balloon Dilation): This procedure involves stretching the narrowed portion of the esophagus to improve swallowing. It may need to be repeated over time.
- Surgery: In some cases, surgical intervention may be necessary to repair severe strictures or complications.
-
Complications:
- Recurrent Strictures: Corrosive injuries can lead to the formation of scar tissue, resulting in recurrent strictures.
- Perforation: Severe injuries may lead to perforation of the esophagus.
- Aspiration Pneumonia: Difficulty swallowing may lead to the aspiration of food or liquids into the lungs, increasing the risk of pneumonia.
Gastritis:
Gastritis is inflammation of the lining of the stomach. It can be acute (sudden and short-term) or chronic (persistent). Gastritis may result from various factors, including infection with Helicobacter pylori bacteria, prolonged use of nonsteroidal anti-inflammatory drugs (NSAIDs), excessive alcohol consumption, or other irritants.
Key Points about Gastritis:
-
Causes:
- H. pylori Infection: Bacterial infection of the stomach lining.
- NSAIDs: Prolonged use of nonsteroidal anti-inflammatory drugs, such as aspirin or ibuprofen.
- Excessive Alcohol Consumption: Alcohol can irritate the stomach lining.
- Autoimmune Reactions: The immune system attacking the stomach lining.
- Bile Reflux: Backflow of bile into the stomach.
-
Symptoms:
- Abdominal pain or discomfort.
- Nausea and vomiting.
- Indigestion or bloating.
- Loss of appetite.
- Belching.
-
Diagnosis:
- Endoscopy: Direct visualization of the stomach lining.
- Blood Tests: To check for H. pylori infection.
- Stool Tests: To detect blood in the stool.
-
Treatment:
- Antibiotics: For H. pylori infection.
- Acid-suppressing Medications: Proton pump inhibitors (PPIs) or histamine H2 blockers to reduce stomach acid.
- Avoidance of Irritants: Limiting or avoiding substances that can worsen gastritis, such as NSAIDs or alcohol.
-
Complications:
- Peptic Ulcers: Gastritis may lead to the development of ulcers in the stomach lining.
- Bleeding: In severe cases, gastritis may cause bleeding in the stomach.
Prognosis: The prognosis for both corrosive strictures of the esophagus and gastritis depends on the severity of the condition, the underlying causes, and the effectiveness of treatment. Early diagnosis and appropriate management are crucial to preventing complications and improving outcomes.
If you suspect corrosive ingestion or experience symptoms suggestive of esophageal stricture or gastritis, seek immediate medical attention for a proper diagnosis and timely intervention.
Category : Corrosive Stricture of Esophagus and Gastritis










